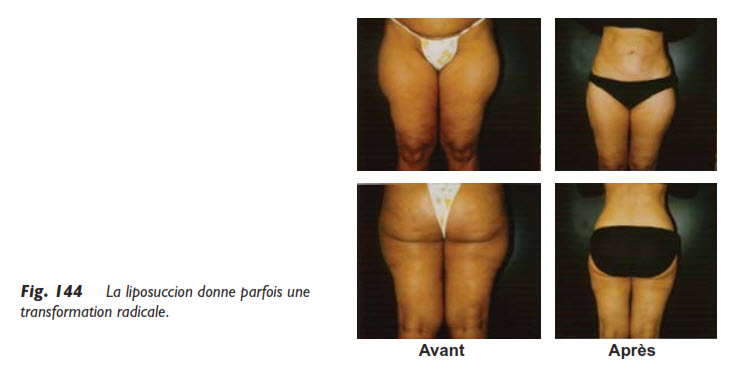
If there is one place where large cannulas should be prohibited, it is certainly the buttocks. Several surgeons refuse to operate on this area because they have achieved poor results, such as sagging buttocks, a curved gluteal fold, skin full of irregularities, or other unsightly complications. This is because they are unaware of the best way to approach this area. In a serious medical journal, the author, a renowned plastic surgeon, admitted that the buttocks were a forbidden zone for liposuction. He should have titled his article: “The buttocks are a challenging area for liposuction, but not forbidden. Inexperienced surgeons, please refrain.”
Here is the procedure for sculpting beautiful buttocks:
Carefully assess the work to be done, by drawing diagrams that clearly map out the so-called severity zones and the grazing zones;
Use fine cannulas, never exceeding 3 mm in diameter;
Work in the direction of gravity, not transversely, which could lead to skin irregularities, i.e., waves.
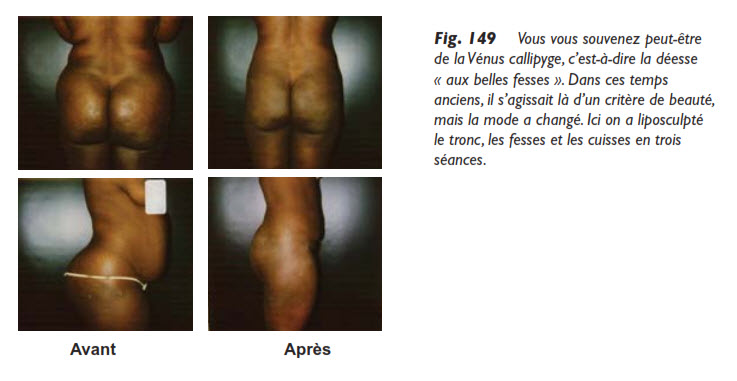
Unlike the saddlebags, where one must flatten an exaggerated roundness, for the specific area of the buttocks, it is necessary to preserve a beautiful roundness that is characteristic of a natural curve. A flat buttock would not at all meet the current criteria of beauty.
The defect that patients often complain about is located at the “apple” of the buttock, as it is commonly referred to in popular language! It is a bump at the infero-lateral part of the buttock that becomes more pronounced with age, responding to the laws of gravity. Over the years, the weight of the buttock, both muscle and fat, causes the buttock to deviate outward. Obviously, diligent exercise will prevent the muscular portion of this problem, but judicious liposuction can address the fatty portion. I say judicious liposuction because the gluteal muscle is a large muscle, responsible for a significant part of the buttock. The surgeon must take this into account and not believe that the buttock is a bottomless pit of fat that can be aspirated at will. Forgetting this could result in nothing less than flat buttocks.
Due to the weight of the gluteal fat, nature has provided ligaments that hold the buttock in place; these are the Jacques ligaments. The female breast also has similar ligaments, called Cooper’s ligaments.
With age and the weight of the fat, the same goes for the breast; these ligaments lose their elasticity, and their gradual relaxation leads to a sagging of the buttock, especially the apple of the buttock. Liposuction will relieve these tired ligaments by allowing the buttock to regain its position. I do not say rise, because the buttock does not rise spectacularly, unlike the abdomen, which will always continue to surprise me.
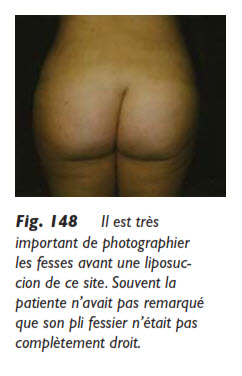
However, these ligaments make the buttock more sensitive, which is why it must be very well anesthetized; otherwise, a slight sensation of electric shocks will make the liposuction unpleasant for the patient. Before the procedure, it is important to have a photo that clearly shows the gluteal fold, as it is not always perfectly vertical due to a hip problem, one leg being shorter than the other, or simply an anatomical defect. Sometimes, it is noticed that one buttock is lower than the other. Most often, patients had never noticed these slight defects, and without this photo evidence, they might mistakenly believe that the liposuction caused this imbalance.
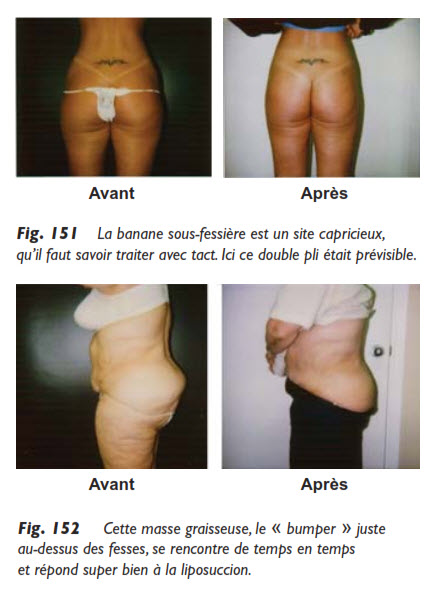
Another peculiarity that is sometimes encountered is that the fat does not seem to have been placed in the right place on the buttocks. The buttock is flat, very cellulitic, and at the sacrum, just above the buttocks, there is a mass of fat, sometimes significant and unsightly, which I have disrespectfully nicknamed “the bumper.” It is as if the fat, by a whim of nature, never descended to its proper place.
Liposuction will do a great service by permanently aspirating this excess, restoring a much more natural contour to this region. The buttock will not be corrected since it is not touched, but it will appear less flat, freed from this fatty protrusion. To correct gluteal cellulite, one can also use a special cannula called “Toledo,” which cuts the adhesions responsible for the cellulite in place. (cf fig. 152)
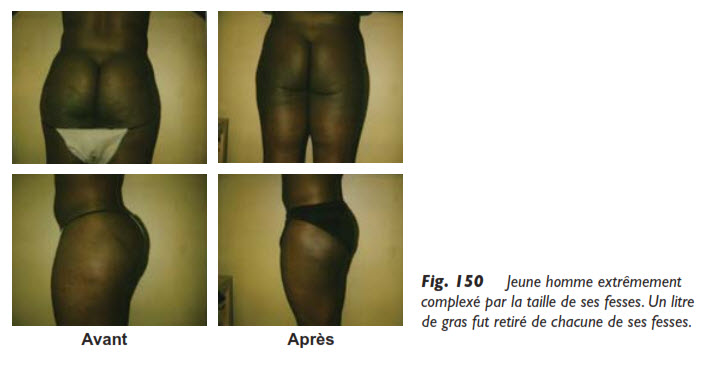
The distribution of fat on the body is genetic. Women of African descent are particularly endowed in the buttocks area, and I have sometimes removed nearly a liter of fat from each buttock, with excellent results. The position of the patient during the procedure is particularly important for the buttocks if one wants results close to perfection. This is why, when I ask my assistant: “Take the buttock position!”, she understands very well that the patient must be lying face down, with a special cushion under her pelvis, which places the buttocks well in view and allows the cannula to reach every nook and cranny. We have already discussed the sub-gluteal banana with the thigh, since this banana forms the junction between the thigh and the buttock. Here, the subcutaneous work is still of great precision.
The treatment of this banana requires a lot of finesse, as it is partly a support for the buttock in addition to the Jacques suspensory ligaments, but I add that if the liposculptor approaches this anatomical site too cavalierly, by not staying superficial with the cannula, he may cause the buttock to sag or create a double or triple fold with the sub-gluteal fold, more scientifically called the gluteal fold.
As I have already mentioned, each anatomical site has its “quirks,” and it is the way the liposculptor handles all these delicate areas that will determine the perfection of the results.
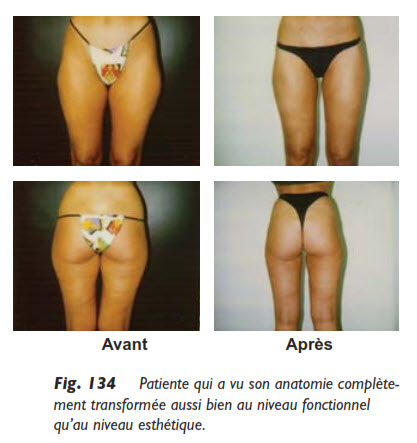
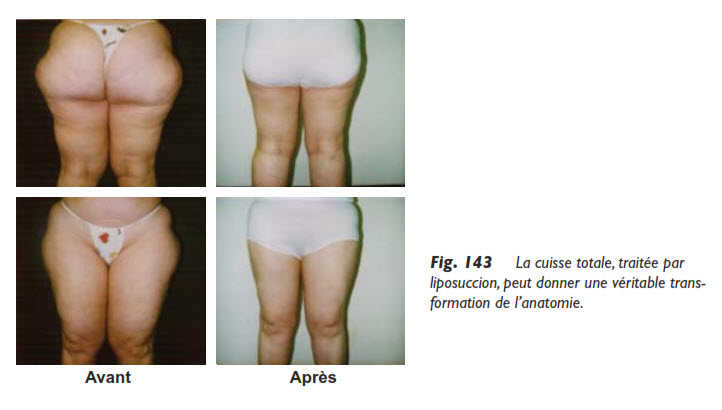
Full thigh liposuction is a very beautiful procedure that can change a life, but it requires the surgeon to have great experience and flawless execution skills because both thighs must not only be slimmed and improved but also identical.
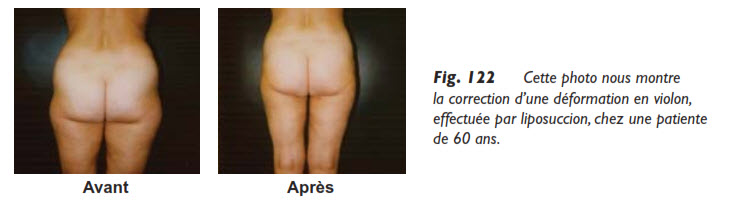
This is entirely possible, and for my part, I have successfully liposculpted hundreds of full thighs to date. Of course, the younger the patient, the easier the procedure and the more predictable the results. The tissues are firm, the skin is toned, and the results will confirm this, as a consequence. I have even performed this procedure on women aged 60 and older with very appreciable results. They only expressed one regret: having waited so long to have the thighs they had always desired. However, in older patients, a more conservative approach is needed for the inner part of the thigh to avoid creating sagging skin.
The outer side of the thigh, having already been explained above with the violin deformity, we will focus on the three other sides of the thigh: the inner, anterior, and posterior sides.
The Inner Thigh
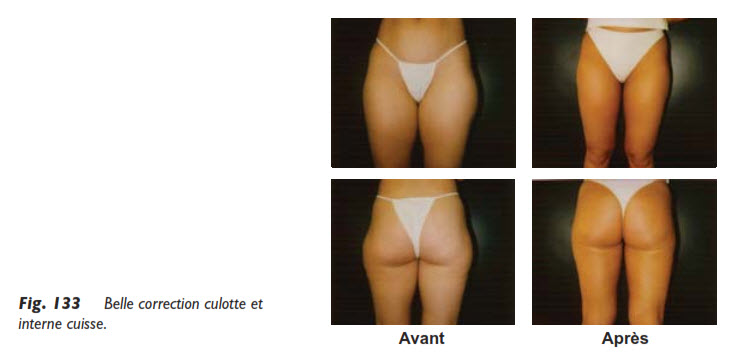
The inner thigh is a site that the English would say. Several surgeons refuse to tackle it, having obtained very poor results and mistakenly believing that this region is impossible to liposculpt. They are wrong because this site sculpts very well and gives magnificent results. The trick: hold the cannula like a violin bow and play it gently. The inner thigh loves a serenade!
This site is further subdivided into three sections that must be approached differently, remembering that in the inner thigh, the fat is devoid of fibers and resembles jelly. Once observed, it aspirates so easily that it is easy to overdo it. The result will be disappointing, which an experienced surgeon will avoid. On the other hand, this lack of fibers makes it an excellent fat when you want to reinject it into an area where it is lacking. Therefore, we have here:
the upper third or the bulge;
the middle third or the groove;
the lower third or the knee.
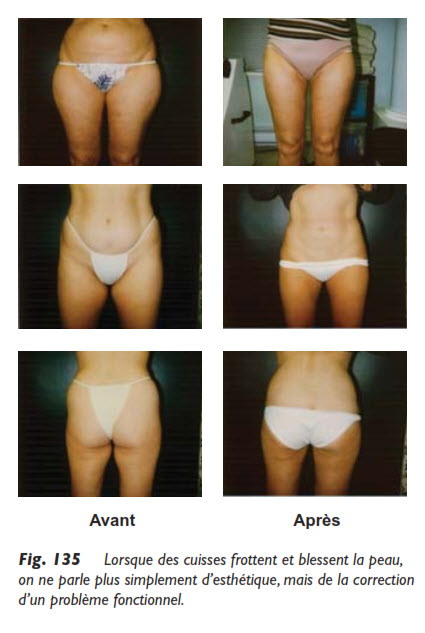
The upper third or bulge of the thigh is a privileged site for liposuction, easy to perform with good results, sometimes even with sagging or aged skin. The secret is to work superficially and remove enough, as patients feel a visceral hatred for this fatty site, which becomes particularly unsightly with age. Moreover, the improvement is felt daily, as when the thighs rub against each other, these people experience a real ordeal. A procedure as benign as liposuction relieves them of this discomfort forever, without leaving the slightest scar, since a “cunning” surgeon can make the incision in the pubic hair and thus leave no trace of their passage. I must admit, however, that pubic hair is disappearing, and this little trick is becoming less and less possible.
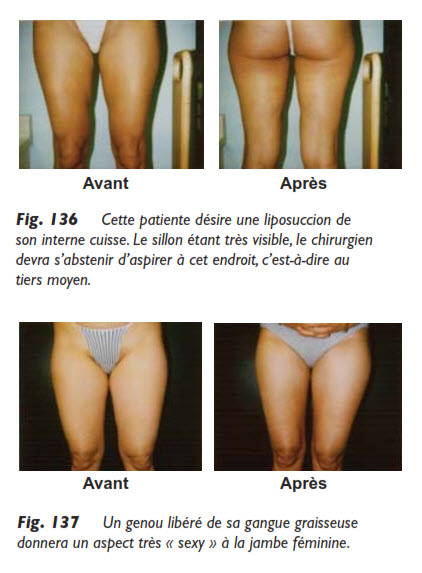
The middle third or the groove often has a depression that must be wary of if you want to correct this flaw. Sometimes, if the groove is very visible, it is necessary to completely refrain from aspirating at this location or to touch it barely, just to make the link between the other two thirds.
The position of the patient on the operating table is also very important to achieve a result close to perfection. It is all these small details that will make patients happy, thanks to results that meet their expectations.
The lower third, that is, the knee, is a site that requires caution because, again, since we are on the inner thigh, the fat devoid of fibers will aspirate very easily. However, well liposculpted, the knee will be particularly beautiful and will give a very nice leg. Moreover, the skin heals very well at this level, and the incisions leave virtually no visible trace.
A patient very satisfied with her knee liposuction found, however, that when she crouched, her knees looked less natural. I explained to her that it is the crouching position that is less natural and that she had the choice of having magnificent knees 999 times out of 1000, or once out of 1000, when she crouched. This anecdote makes you smile: a liposculptor must know how to negotiate this kind of argument.
On another occasion, I had removed a very unsightly saddlebag, and the patient came back to see me six months later to tell me that when sitting on the toilet, her outer thigh took on a strange shape, but otherwise, she was still as happy and satisfied! I had to spend half an hour convincing her that she had the choice between super thighs all day or, when sitting on the toilet, a less pleasant profile to look at…
Should we just move the mirror?
The Anterior Thigh
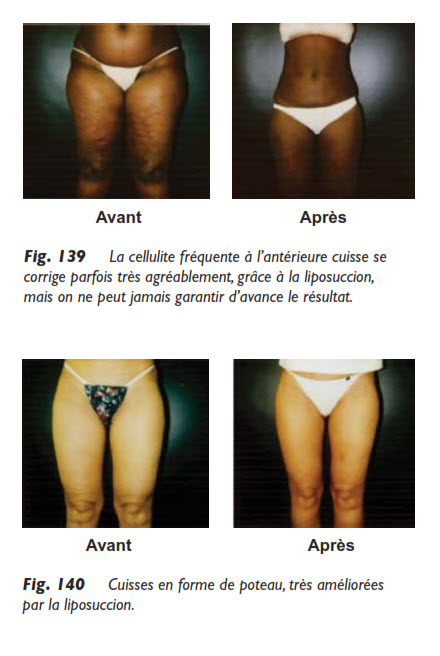
The anterior thigh is a site that is not often involved. Indeed, it has certain pitfalls that the experienced liposculptor will know how to avoid. First, the patient looks at the front part of her thighs from above and sees herself differently from reality, since in the eyes of others, it is from the front that she shows her thighs. The patient, when looking in the mirror, no longer sees the flaws she saw from above or sees them differently. She then believes that it is the lighting that distorts reality or the perspective of her own height while she tries as best she can to explain to the surgeon what she does not like about the front part of her thighs. It could be waves, holes, bumps, skin irregularities, or simply an accumulation of too much fat at this level.
Here is the course of action:
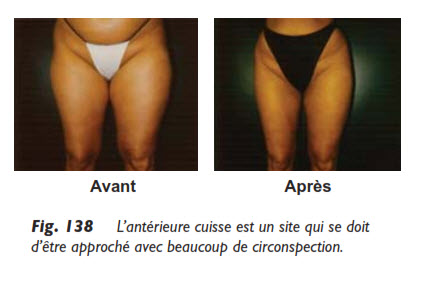
When the anterior thigh is too fatty, it can be liposculpted, but on the condition of never removing more than 50% of the fat and using very fine cannulas no larger than a knitting needle (3 mm). Otherwise, skin irregularities may occur, and this is a site that does not forgive.
If the anterior thigh is not too fatty but really presents what the patient saw from above, it may be a bit cellulitic. To the point where sometimes patients refuse to wear shorts. At that point, it is possible to simply use a special cannula (Toledo or Blugerman) that loosens the skin without aspirating fat, with the hope of improving this cellulite, which is due to multiple adhesions as I have already explained.
However, the degree of improvement of this cellulite cannot be predicted with certainty, and it is important to explain this in advance to the patient, as this type of improvement is not as predictable as pure and simple liposuction. When leaving this very particular site that is the anterior thigh, let’s mention the upper part of the knee, which is often plump. Although not easy, an experienced surgeon will manage to level this area well, without leaving traces of their passage.
The Posterior Thigh
This time it is true, with very rare exceptions, the posterior part of the thigh is not well suited for liposuction. First, the fat is generally very thin there, and venturing there could lead to skin irregularities.
Moreover, from a medical-surgical point of view, if we treated all four sides of the thigh in the same session, that is, the entire circumferential thigh, we could have serious complications of phlebitis due to a “tourniquet effect,” that is, postoperative edema that would trap the thigh by obstructing circulation.
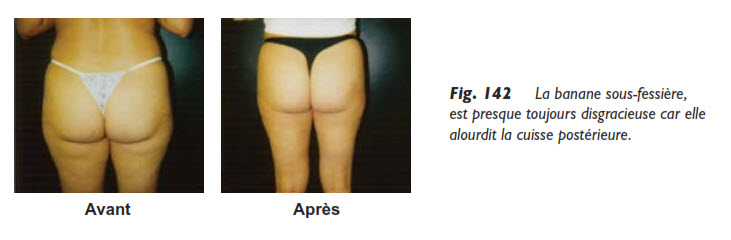
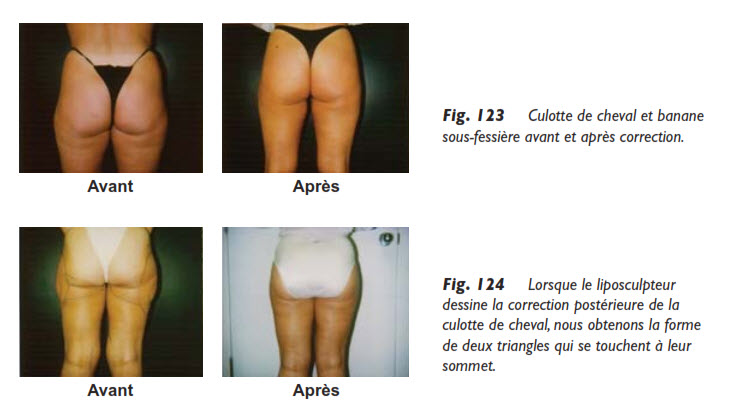
On the posterior thigh, we limit ourselves to operating on a thin portion, located just below the buttock, and quantitatively insignificant, called the “banana” under the buttock.
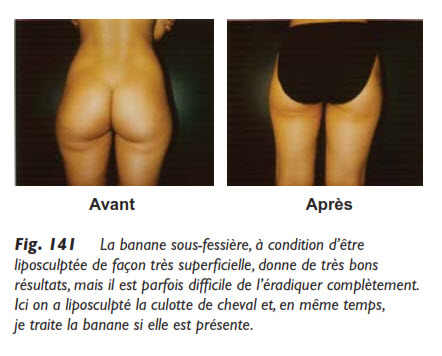
The “banana” under the buttock is particularly unsightly in some and deserves to be aspirated. Moreover, I always include it when I operate on a saddlebag. Again, allow me to use the English word, as the banana has a very useful anatomical role, as it supports the buttock, and if it were removed too radically, it would produce a sagging buttock, worsening the situation rather than improving it.
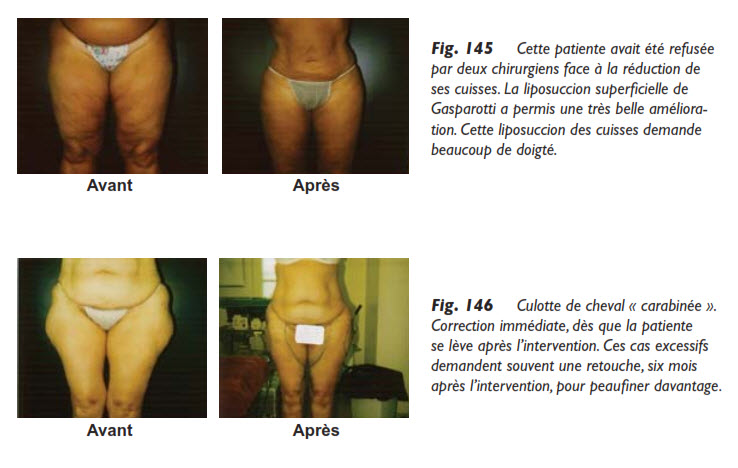
But rest assured, the experienced surgeon will proceed very superficially at the level of the “banana,” to refine this particular site. I am convinced that the superficial liposuction technique of Gasparotti, which I have already mentioned, applies everywhere on the body, but for the “banana” under the buttock, this technique is a “must” if you want results close to perfection. While slightly reducing the posterior thigh, the disappearance of this banana under the buttock improves the visual effect in a very beautiful way.
The Total Thigh Viewed from Different Angles
The total thigh can present all kinds of peculiarities that the liposculptor must face while remaining very creative.
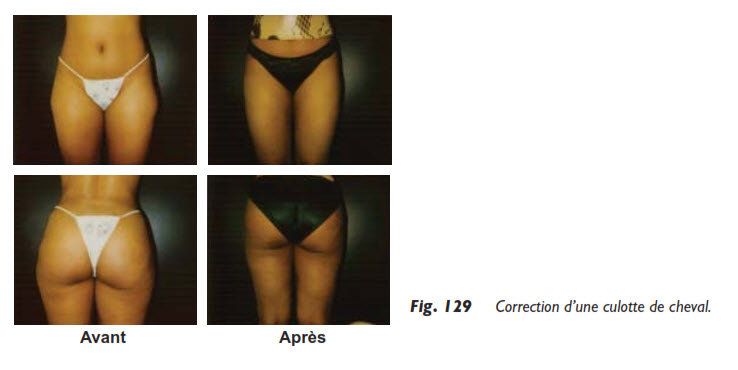
After the abdomen, the most popular liposuction procedure is undoubtedly the upper lateral thigh, also known as saddlebags. The flank just below, better known as love handles, also brings its share of dissatisfaction. This is why I treat these two areas as a single anatomical unit, and when the patient comes for her saddlebags, I encourage her, when indicated, to address both at the same time. Why correct only one flaw and leave the other for later, when both can be removed simultaneously at a lower cost, completely resolving the issue?
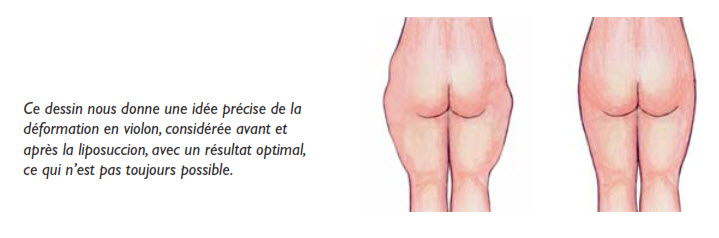
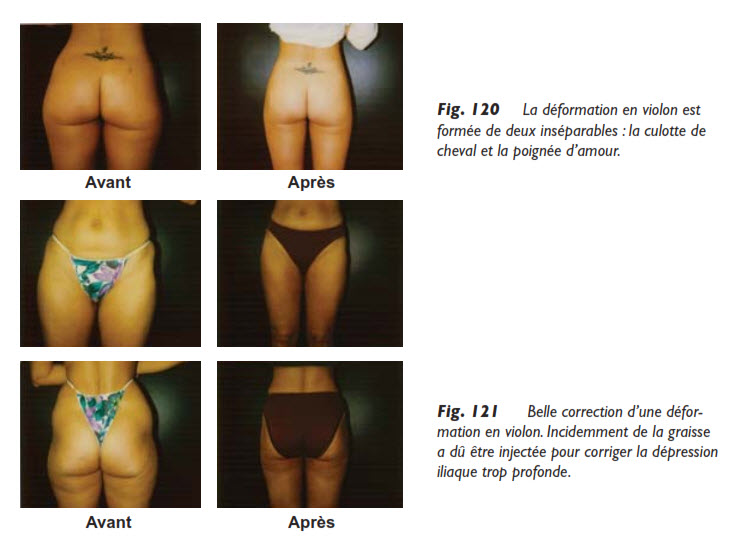
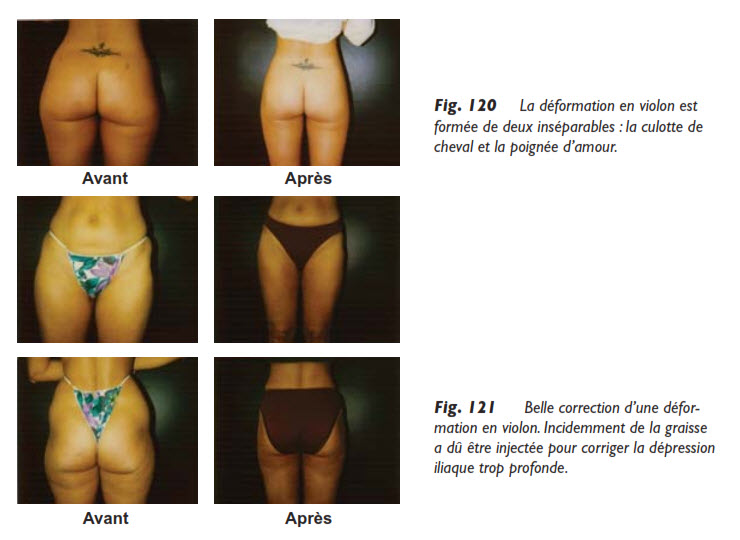
As we touched on in a previous chapter, the violin deformity combines three anomalies:
saddlebags;
love handles;
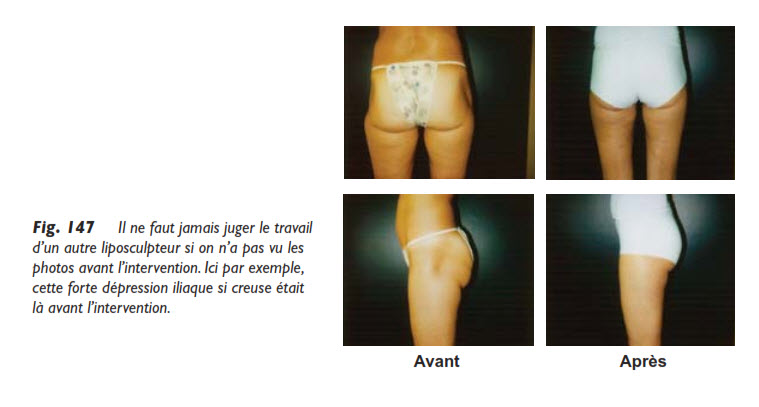
a more or less hollow area between these two fat bulges, known as the iliac depression.
However, note that while three anomalies contribute to the violin deformity, its correction must go beyond these three anomalies. Indeed, experience has taught me that to achieve an excellent result, it is necessary to correct the lower buttock and the banana, that is, this banana-shaped fat bulge on the upper posterior part of the thigh.
Indeed, the weight and volume of the fat in these two areas, the buttock and the banana, push the thigh outward, accentuating the saddlebags. I have named these two areas the triangle, because when drawing on the patient, it forms a triangle.
However, note that while three anomalies contribute to the violin deformity, its correction must go beyond these three anomalies. Indeed, experience has taught me that to achieve an excellent result, it is necessary to correct the lower buttock and the banana, that is, this banana-shaped fat bulge on the upper posterior part of the thigh.
Indeed, the weight and volume of the fat in these two areas, the buttock and the banana, push the thigh outward, accentuating the saddlebags. I have named these two areas the triangle, because when drawing on the patient, it forms a triangle.
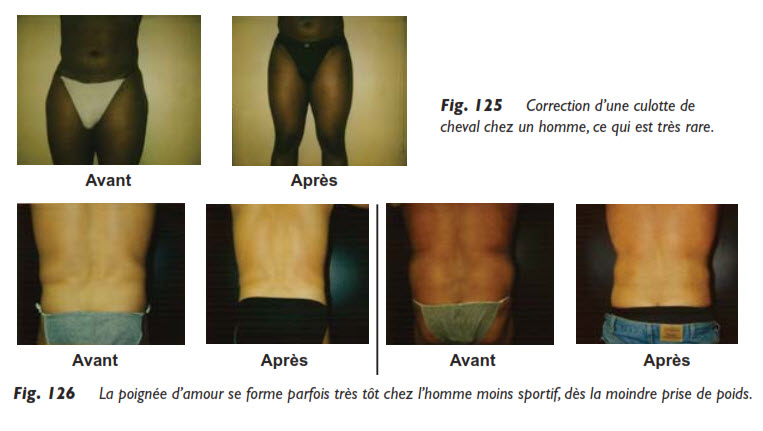
Fatty flanks or love handles are almost always present, especially since they tend to increase in volume after menopause. Reducing them through liposuction can be a true rejuvenation. It is important to note that love handles are very common in men, and this aspect leads to constant demand for liposuction with excellent results, but it requires a reliable technique since the fat there is very fibrous and harder to remove.
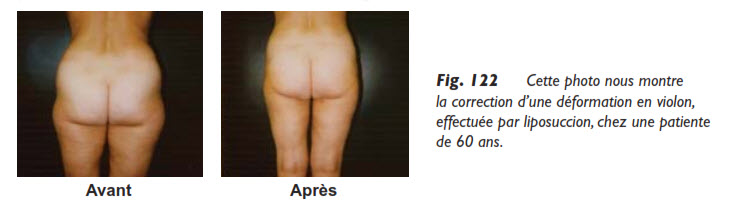
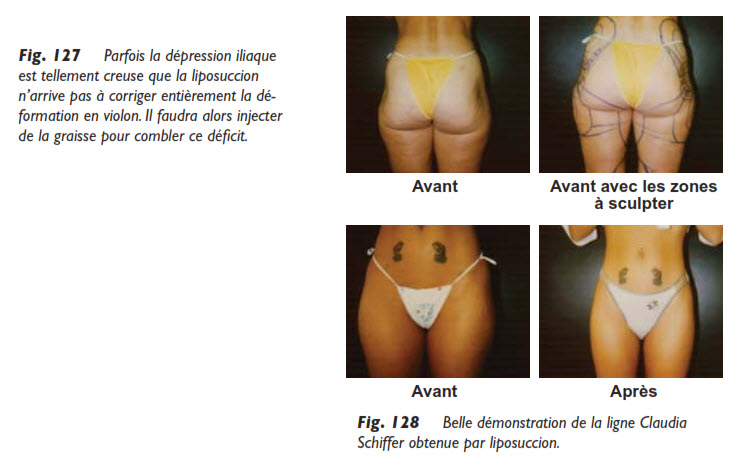
The iliac depression, this hollow area between the two bulges of the violin deformity, is sometimes completely devoid of fat. At that point, we start by harvesting fat from the outer thigh or flank, and at the end of the procedure, we reimplant this freshly “harvested” fat to fill the hollow area. Then, with their thumbs, the surgeon molds this new fat, as if it were modeling clay, to distribute it evenly.
Since the reinjected fat does not fully revive, some can be stored in the freezer to be reimplanted a few months later. At that point, we hope to achieve the line I have named the “Claudia Schiffer line,” which is a harmonious, perfect curve running from the flank to the outer knee, without any breaks or bumps. Returning to the saddlebags, the first of the inseparable duo, let us repeat that it was this area that motivated the invention of liposuction. Indeed, large bellies, especially aprons, were treated by lipectomy, despite unavoidable scarring, but at least with clothing, the disfigurement was no longer visible, except in private.
For saddlebags, the operation was much less suitable, as the fat block to be removed was harder and less well-defined than an apron of fat; also, the procedure caused such scarring that the patient could hardly show her thighs anymore. Then came liposuction…
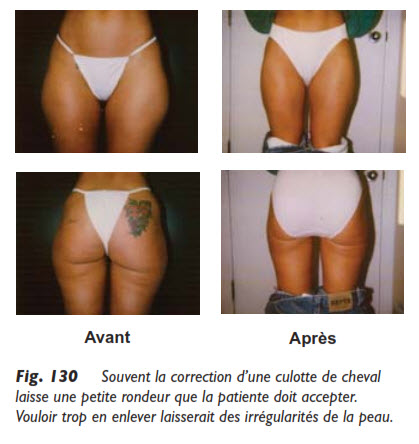
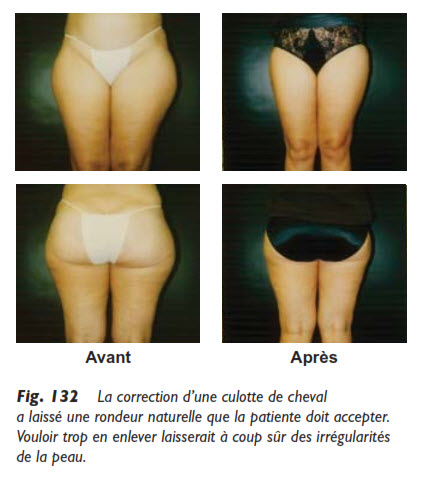
But what the patient must understand once again is that liposuction only accesses fat. If the muscle is “bulging” in that area or the bone is prominent, some roundness may remain, although the improvement will always be significant. Of course, some patients will not be satisfied, even with excellent results, because they wanted to look like a friend who went to a certain surgeon and was left with no roundness at all. But would that other surgeon have done better? Each patient is different, and trying to remove too much to flatten the area at all costs would lead to skin irregularities, very unsightly, somewhat resembling repoussé leather.
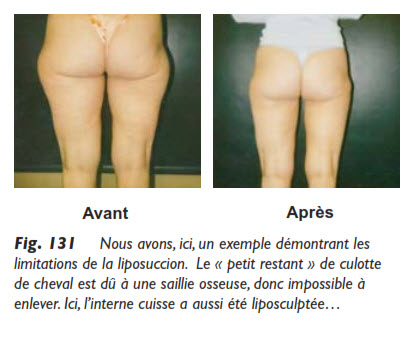
I take advantage of this photo (Fig. 131) to express some reservations about comparisons between different practitioners. Despite my experience of over 5000 procedures, I can never offer a patient an absolute guarantee of the outcome of a liposuction. What I know for sure is that the quality of treatment, the attention paid to patients, and their motivation to improve their appearance for many years guide every professional action I take in the most transparent dialogue possible.
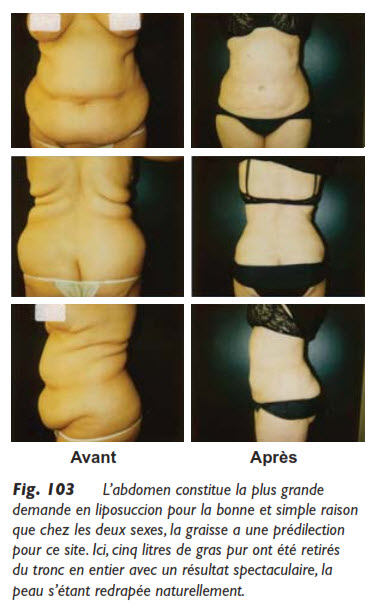
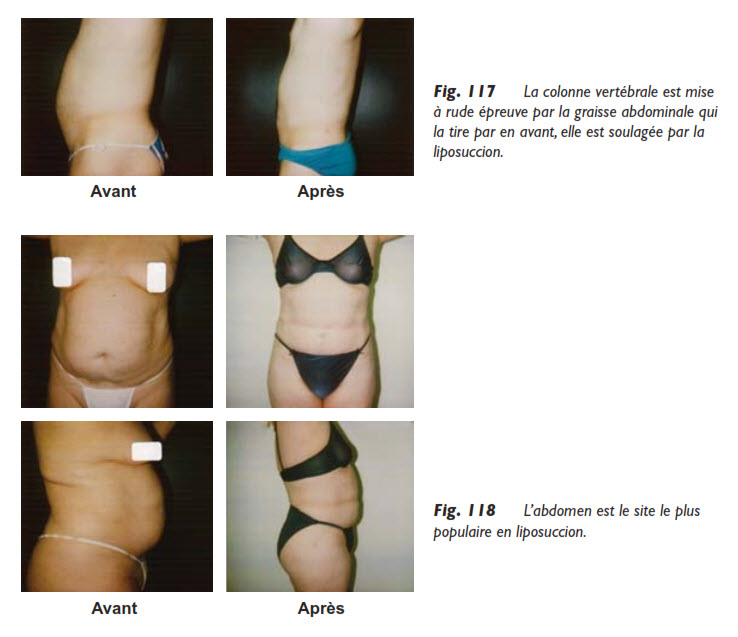
The abdomen is the most targeted area for liposuction. It far exceeds all other treatment areas by a significant margin. This is primarily because this area concerns both men and women, which is not the case for the thighs or buttocks, where male demand is almost non-existent. Secondly, due to post-pregnancy effects, android obesity, and hereditary factors, women are often affected by excess fat in the abdomen. Fortunately, the skin of the abdomen is of exceptional quality, especially in women, so the aesthetic results are impressive, as the skin can naturally retract afterward.
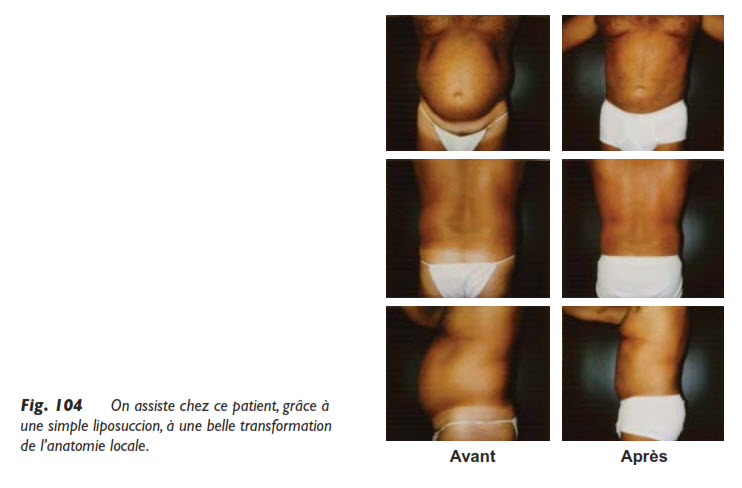
Liposuction provides an effective solution for individuals struggling with excess fat in this area, even in older individuals who have accumulated significant abdominal fat over the years. I even recounted a case where I had to perform the procedure in two phases, operating on the left side first and then the right side two months later, removing about four liters of fat each time. Additionally, there is another, less anecdotal way to perform the procedure in two phases on the abdomen. First, the area below the navel, or the hypogastrium, is treated, followed by the area above the navel, or the epigastrium. This is done, of course, when the abdomen is too large to be treated in one session, which is very rare.
It is important to note that the abdomen is a unique area that requires specific anatomical knowledge, both superficially and deeply. Superficially, the abdomen is divided into four regions that the liposculptor must understand well, especially to explain them clearly to the patient.
The epigastrium or upper abdomen, which patients often refer to as the stomach;
The hypogastrium or lower abdomen, which most people call the “belly,” and which can sometimes be complicated by an apron of fat;
The periumbilical region, which must be well sculpted, otherwise it may look like a donut;
The central part, which can be called the waist; this part connects the upper and lower abdomen.
Why are these anatomical considerations important? To know exactly which area is being discussed: sometimes liposuction will only target the lower abdomen, more rarely only the upper abdomen, but most of the time, the entire abdomen will be the focus of the procedure.
It is very important to emphasize here that liposuction cannot correct a large belly caused by loss of muscle tone. It is equally important, during the consultation, to make a proper diagnosis and to clearly explain the ins and outs of the procedure. The surgeon’s honesty is always extremely important, especially in liposuction. A patient will always be very grateful for being fully informed before the procedure, allowing them to make an informed decision.
As I have already mentioned, the diagnosis here is very important, especially in cases of very prominent abdomens known as “hard belly.”
Indeed, this prominence is caused by visceral fat, located behind the muscle, which, being extremely acidic, accentuates this belly. Of course, the liposculptor has no access behind the muscle. It could be said that this muscle no longer contracts, like an overstretched elastic band. Therefore, liposuction is impossible in the case of a hard belly.
It is easy to understand the importance of muscles in the shape of the abdomen, particularly those that form the abdominal belt, often called the abdominal girdle.
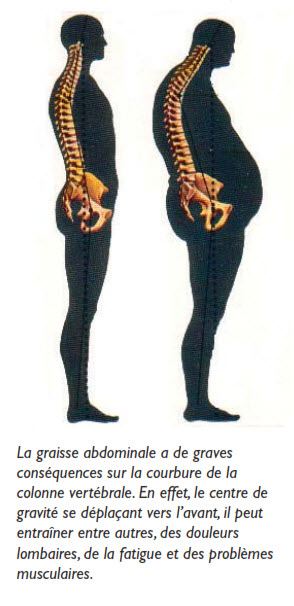
When these muscles are too weak, the weight of the viscera plus the surrounding fat pushes the belly forward, excessively increasing the “hollow” of the spine, often causing back pain, specifically in the lumbar region.
With liposuction, possible when the fat is located between the skin and the muscle, the relaxation caused by the weight of the fat is corrected, and at the same time, the spine is relieved.
It is common that immediately after abdominal liposuction, when the patient stands up for the final check, a straightening of the spine is immediately noticeable, which is a pleasure to see.
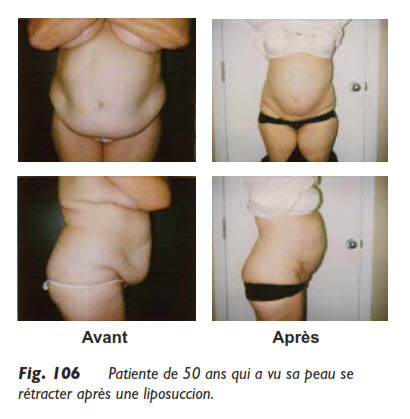
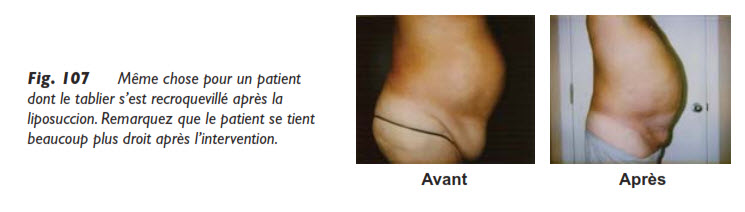
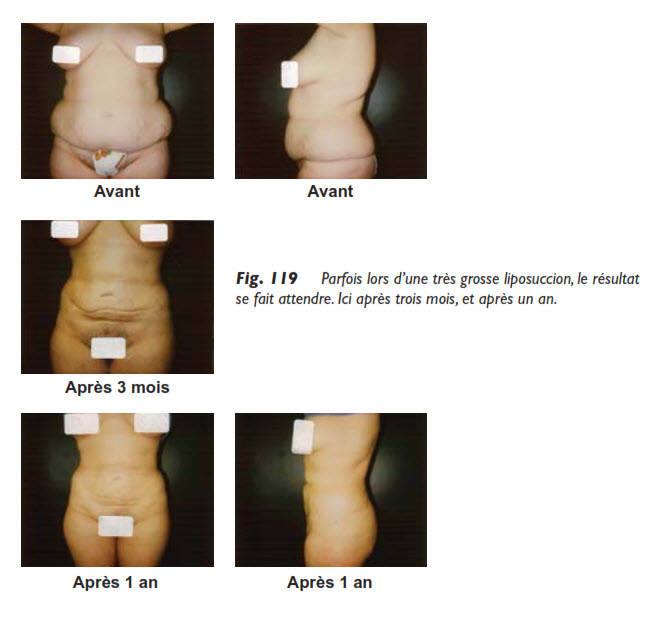
Some people come to the consultation with a very significant fatty apron, sometimes even covering the pubic area. What will happen to the skin after the procedure? Well, believe it or not, thanks to the superficial liposuction technique already described, the skin will retract. Of course, it may not retract completely, but there will always be a noticeable improvement. I have observed aprons of 8 inches (20 cm) in length reduced to just half an inch (1 cm) after liposuction, as it is important to reiterate that it is not the skin that causes the fat to sag, but the fat that causes the skin to sag: if this fat is removed, the skin will return to the place it should have always been.
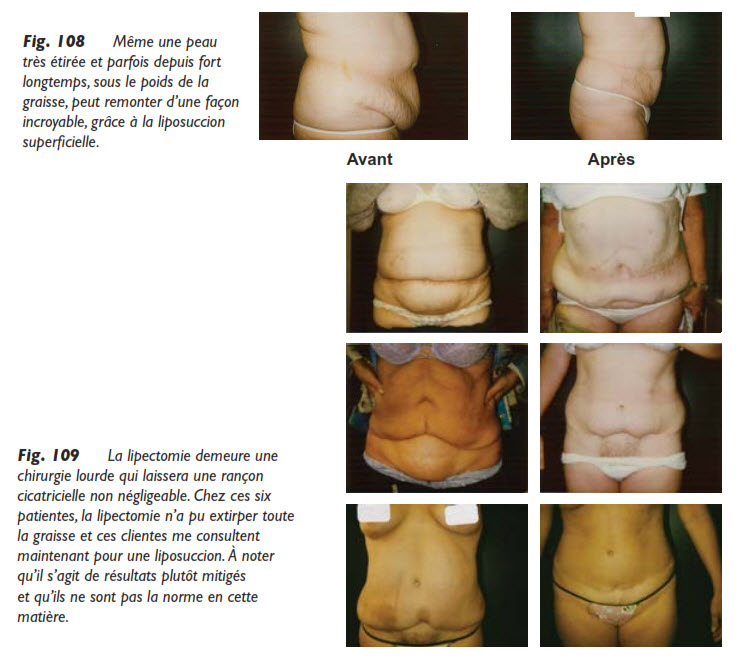
In the past, a lipectomy (surgery for the fatty apron) was performed immediately in such cases, but today, with the development of liposuction, most professionals agree to start with liposuction, and if the skin does not retract enough afterward, which is rare, it would be easy, during a second procedure, to remove this slight excess of skin.
Liposuction is a benign procedure compared to lipectomy, which is a more invasive surgery and therefore more prone to side effects. Moreover, lipectomy, which involves removing a large block of fat and skin with a scalpel, often leaves an unsightly scar, an artificial navel, and cannot remove fat as effectively as liposuction.
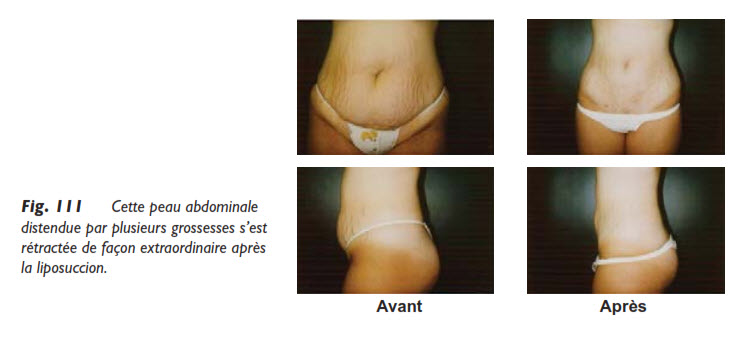
Another noteworthy fact is that the abdominal skin, especially below the navel, is of exceptional quality. Let’s not forget that this skin stretches multiple times during pregnancies and retracts perfectly after childbirth. You often see women who have had four or five children and still have a beautiful belly.
Therefore, this abdominal distension is often strictly due to the volume of fat, which, once treated by liposuction, will allow the skin to retract very adequately.
Often, a horizontal fold can be seen at the level of the navel, dividing the abdomen into two parts, the upper and lower, due to a local anatomical peculiarity, the Camper’s fascia. I then warn the patient that this fold will persist after liposuction, but less deeply.
In fact, as I have already explained, and I will repeat because it is so important, the abdomen consists of three layers or levels:
The fat located between the skin and the muscle, the target of liposuction;
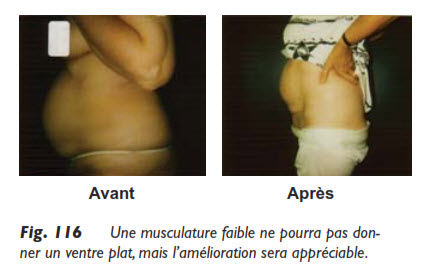
The muscle, which is sometimes in very poor condition, having lost its tone;
The omental or visceral fat, located behind the muscle, at the level of the intestines.
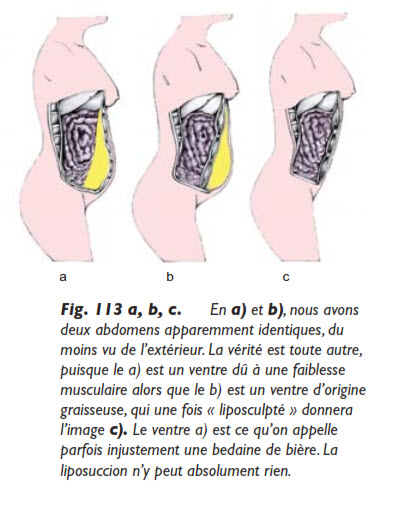
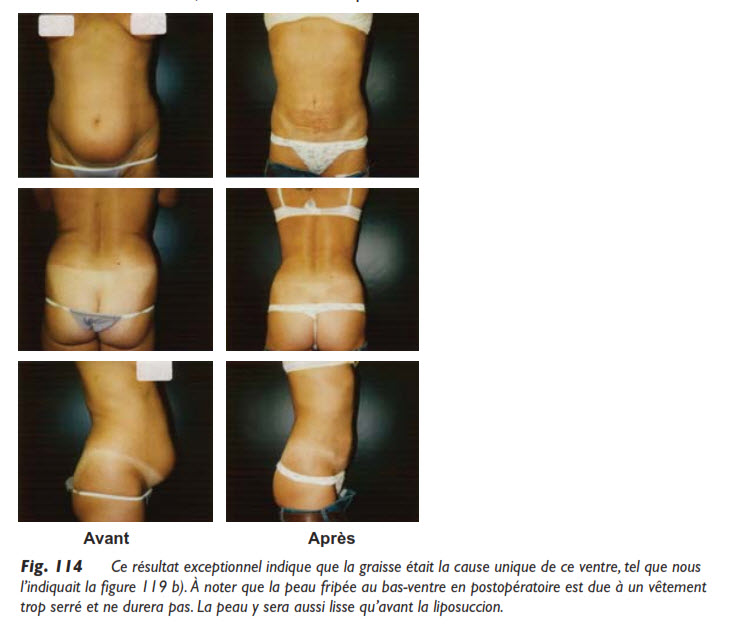
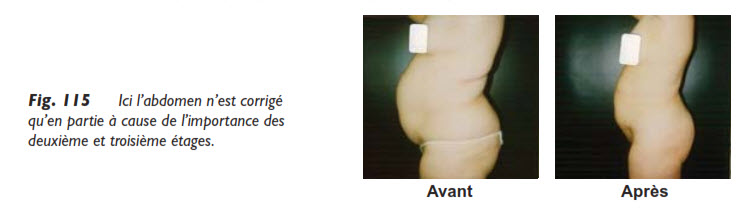
When faced with a large belly, the liposculptor must perform an examination to assess the importance of each of the three layers. The more significant the first layer is (e.g., b), the better the liposuction results will be. In other words, if your fat is in the right place for liposuction (i.e., just under the skin), the results will be positive.
Very often, a large belly is a function of the three layers, for example, 50% first layer (that’s where the action is), 25% due to weak abdominal muscles, and a final 25% due to fat located behind the muscle. In such a case, in addition to liposuction, abdominal muscle exercises will be needed for the second layer and a diet for the third layer. This way, optimal results can be achieved.
If the large belly is 100% due to fat located between the skin and the muscle, then liposuction will give you a flat belly, like a pancake. It is during the consultation that the importance of the “first layer” must be well evaluated in relation to the other two. The patient must know in advance what kind of belly they will have after the procedure. This belly will be reduced by half, three-quarters, or completely, depending on the importance of the first layer. And the surgeon must not only say it but also write it on the consent form. Why? Memory, as we know, is a faculty that forgets. And a disappointed patient will quickly blame their liposculptor, rightly or wrongly. Or perhaps rightly if the pre-operative explanations were incomplete.
Liposculpture is a precision job that requires a lot of concentration and inner peace, which does not go well with patient complaints. However, good news, I have sometimes achieved surprising results, even with a less significant first layer, because aspirating this first layer of fat relieves the muscle, which is less stretched forward. Understand the situation of the abdominal muscles. Caught, so to speak, between two fires, they are pushed forward by the intestines and visceral fat, and in addition, they are pulled forward by the subcutaneous fat. This push-and-pull effect exerts tension on the spine, seeking to pull it forward as well, and consequently, to hollow the back, causing uncomfortable and sometimes painful lordosis.
Some patients prefer to wait until after childbirth to get rid of their abdominal fat, mistakenly believing that this is better. What a pity for them! All those years lost before achieving the waistline they desire. Waiting only increases fat deposits, and liposuction will only be more significant after the second or third child.
If, on the other hand, liposuction is done early, the fat cells, once aspirated, will not return, and the new waistline will be more easily achieved after each childbirth.
In short, liposuction can significantly contribute to restoring the body’s natural contours, without performing miracles. This discipline involves transforming the contours without changing the bone and muscle structure. Thanks to microcannulas and tumescence, this art has reached a very high level of refinement, offering much hope to those who suffer from disproportions related to fatty tissue.