On the day of the procedure, you arrive very relaxed since the night before you were prescribed a mild sedative to ensure a restful night.
When you arrive at the clinic, you are first greeted by a nurse who asks you to complete a short questionnaire, then takes your vital signs and other tests (blood sugar, pregnancy) before inviting you to change into your surgical attire.
Next, the doctor meets with you and after examining you, reviews the areas to be liposculpted, takes measurements of these areas, and photographs them. This contact is very important, as it also allows you to anticipate the results.
Often intimidated by the photo-taking, patients may feel embarrassed. These photographs are crucial, as the surprise of patients is beautiful to see when they look at these photos three months after the procedure. Most of the time, the adaptation to their new shapes is so pleasant and gradual that patients admit they have no memory of ever having had this appearance in their past.
It is important that these photos are developed immediately so that they can also be consulted during the procedure. Indeed, the fatty tissues at that time will be distorted by the lying position and by the large amounts of anesthetic liquid infiltrated into the fat.
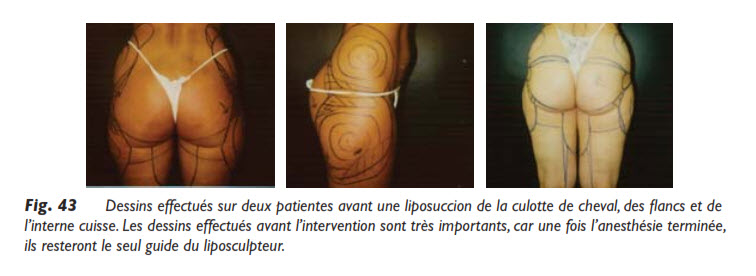
The areas to be liposculpted, clearly drawn with a marker pen on the patient in a standing position, resemble a topographic map. These drawings will be the inspiration for the liposculptor, his precise guide for each area where he will have to exercise his art.
The areas to be liposculpted must be well defined. Using concentric circles, the surgeon indicates where the “top of the mountain” and the “bottom of the valley” are, because once the area is infiltrated, this is the only reference that will remain with the preoperative photos, which must be displayed clearly.
We create with pluses and minuses, a mapping of the areas to be aspirated more or less severely, in order to obtain the most harmonious shapes possible.
The areas to avoid, or those needing filling, will also be very well indicated. This is why the drawings may differ from one side to the other, as for most of us, we are not identical on both sides. If there are sometimes irregularities on the skin, such as small depressions, waves, or cellulite, it is good to indicate them, among other things, so that these defects are not later attributed to the surgeon. Each body is unique and must be treated as such: the bone structure, skin elasticity, hollows and bumps, very frequent asymmetries, muscle tone, and so on…
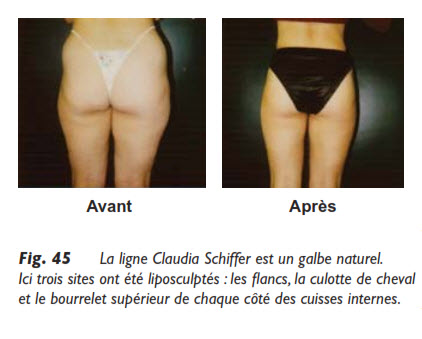
The diagram must indicate in detail the areas where the fat is thickest and also thinnest, in order to correct the local anatomy, that is, to remove excess fat and leave it where necessary. If we aspirated everywhere with the same intensity, we would reproduce the disgrace, but on a smaller scale. Thus, a large violin-shaped deformity would become a small violin-shaped deformity; this is not the desired result. We want to eliminate this deformity and create what I have called the line, that is, a line that starts from the hip and fades to the knee without interruption, drawing a perfect curve.
Once the areas to be liposculpted are well identified on the patient, the nurse is ready to infiltrate them (perform local anesthesia), according to the doctor’s prescription, as it is important not to exceed the permitted doses of medication. Some have done so in California or elsewhere, with consequences that made headlines. It only takes one bad publicity to make patients insecure and cast unfounded doubts on liposuction, as it is a proven and effective technique when practiced according to the rules of the art.
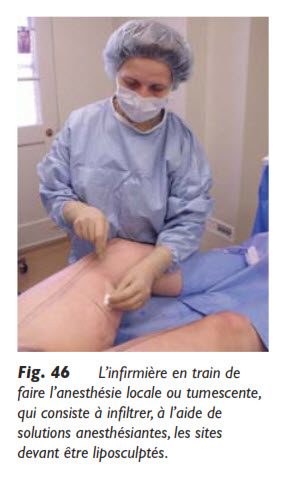
Premedication is given to dispel any lingering anxiety, which would lead to tension and make the local anesthesia uncomfortable. We start by freezing the skin with a very fine needle, which is almost painless. We make small dermal buttons through which it will be easy to insert a longer needle into the fat to anesthetize it. The fatty tissue being poorly innervated, it remains relatively insensitive and anesthetizes very easily in general.
The nurse then infiltrates the fatty tissue with liters of anesthetic, which produces tumescence. The fatty tissue becoming firm, it will then be easy to move the cannula around, while aspirating the fat, without hitting the surrounding tissues. It is very important to infiltrate generously, especially if the skin is flabby, as this stabilizes the area and, once again, facilitates the movement of the cannula and the extraction of fat. Tumescence produces hydrodissection of the fatty tissue and keeps the skin well in place.
The patient remains completely alert and awake, and we chat during the procedure, which lasts a little over an hour for three sites, which is a reasonable average.
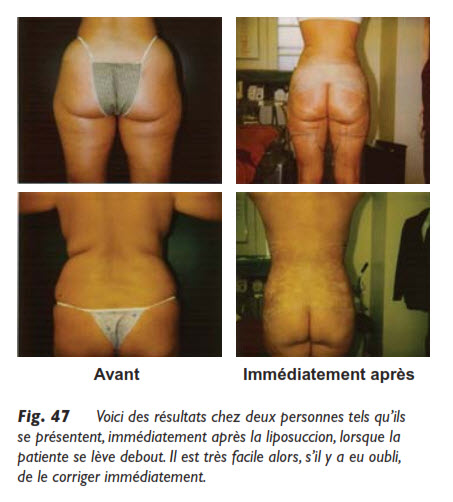
When the excess fat is completely suctioned, the patient is examined again in a standing position, which gives a much more realistic picture of the result. This is where we can see if there is asymmetry, if all the excess fat has been removed, if the skin is smooth, and other observations to proceed with immediate touch-ups if necessary. If the patient had been asleep, this standing examination would have been impossible, and it would only be after six months that we could notice “shortcomings,” and obviously, we would have to touch up, which is not pleasant for anyone!
For my part, after examining my patient in a standing position, it is often necessary for her to lie down again for fine touch-ups that will lead to results that I want to optimize, getting as close as possible to perfection. The result will only be better.
New photos are taken and compared with the first ones, as sometimes we can see details in photos that were not visible to the naked eye.
It will then be very easy to perform a final touch-up immediately, while the tissues are still well anesthetized. In my personal practice, I often reaffirm that this standing examination is a better guarantee of success. This precision work would have been impossible with general anesthesia, and especially the touch-ups could not have been done on the spot!
Already the patient can see the difference between the photos. Sometimes, the emotion is immediate in the face of the positive gaze that is cast. Tears of joy often conclude this examination, which delights both the artist and the model. To conclude, regarding the type of anesthesia, I feel extremely confident when I can discuss with the patient, completely awake and alert, during liposuction.
When he stands up after the procedure, smiling, and can leave an hour later on his own two feet, I feel really safe, because my patient is also safe.
If I call him the day after tomorrow to check on him, and he answers me in a normal voice, going about his usual activities or resting, I am reassured once again that I have not put him in danger, but only helped him appreciate his life.
When everything goes well, which is the norm, two or three days later, sometimes more if it is a major procedure, the treated person can return to work. I observe in this follow-up that I have not endangered his health and that I have acted with great discernment. And this is the way to work in tumescent ambulatory liposuction, at the service of patients with whom trust remains a precious bond.